
The following post was contributed by Jonathan Gadsby.
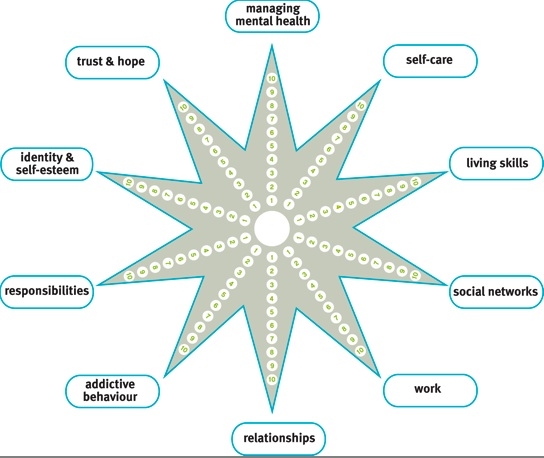
The Mental Health Recovery Star (below) is a widely used tool which aims to provide a map of a multifaceted mental health recovery and a measurement of progress. It was designed by Triangle Consulting Social Enterprise in 2007, a group based in the world of outcome measurement (‘counting what really counts’) and business coaching. The purpose of this critique to explore reasons why we might wish to be cautious about the Recovery Star and its underlying assumptions. It has been prompted by the recent creation of the ‘UnRecovery Star’ by the critical mental health survivor group, Recovery in the Bin.
 Part 1: Some background
Part 1: Some background
There have been a number of attacks on the Recovery Star. The first and perhaps most obvious is that there is a significant potential for it to manualise improvements in mental health, moving towards the idea that wellbeing is something that can be “delivered” by following a relatively simple procedure and moving away from an understanding that there is an essential relationship of trust and empathy. It has been a long-standing instinct of nurses that such a relationship is vital and service-users consistently report that it is being listened to with empathy which they value more than ‘interventions’. That NHS Managers see the Recovery Star as something which can improve the ‘throughput’ of their service while employing a less expensive workforce is also not in doubt, and the very existence of something like the Recovery Star makes its project – ‘recovery’ – more open to becoming a commodity, along with the people it claims to measure. One should set these points (and the ones which follow) against the unfortunate backdrop that there are plenty of mental health nurses whose level of conversation with service users is significantly less skilled and comprehensive than the Recovery Star and whose relationships are not in general characterised by listening, trust and empathy. Also, one could argue that it is possible to use the Recovery Star, or at least aspects of it, as part of a good relationship rather than as a replacement for it. It may be that many people have felt helped through its use and it is not the intention of this critique to invalidate their experience.
A second attack on the Recovery Star comes from a more philosophical angle: in terms of ethics, it is overwhelmingly consequentialist. While this gives it a great practicality, one cannot help but notice that there are moments in which it seems to treat every action and every other person as transactions to be maximised for personal benefit. It would be difficult to imagine using the Recovery Star to ask service users what it would mean for them to be living a good life, a life that matched or helped them to explore their values, a life of meaning and purpose. Somehow fulfilment becomes functioning. Given that deontological ethics are so important to nurses (a code of conduct, Rogerian principles, a duty of care) there is a (frankly sinister) question about whether values are what nurses aspire to but are somehow too good for our service users. We have a rich and principled inner life… but they should stick to the target-setting of self-management. This criticism is one that could be made of services more widely but is very present in the Recovery Star.
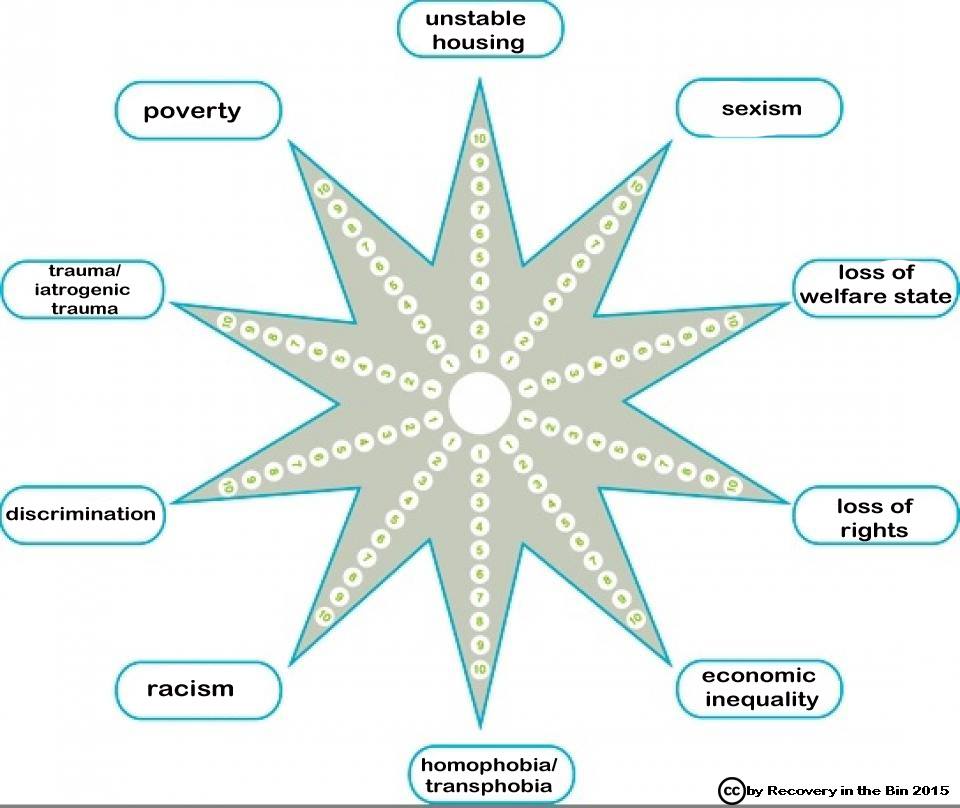 There is a third set of arguments, and they have recently been brought into a sharp focus. Recovery In The Bin is a Facebook-based survivor group, growing in membership and influence. This month they presented at the Making Sense of Mad Studies conference at Durham University. Members have designed another star, the UnRecovery Star (right). UnRecovery is a term which they define in a number of precise ways. It is a project which continues to evolve. Their attack is a political one: far from opening the frames of reference from narrow medical illness to more holistic personal wellbeing, the Recovery Star continues an onslaught of neoliberalism in mental health, in which people are to be made individually responsible for difficulties which would be better thought of as originating in society. Through this lens, the holism of the Recovery Star becomes a complete colonisation of a person with a set of ideas that appear to be liberating but in fact absolve the powerful from the need to acknowledge and address inequalities of all kinds. For example, widening the conversation to include work and financial skills might seem welcome because loss of role, loss of meaningful activity and financial worries are very significant drivers of distress. However, in so doing, we may be failing to notice with the service-user that they live in an unjust society in which finding one’s way and having access to decent housing, meaningful roles, security, having protected rights and simply being allowed to be different seem to be increasingly the domain of the privileged. Being valued in society may be based on assumptions which many nurses may readily agree are insane. Nurses who unquestionably agree with the Recovery Star that mental health is synonymous with self-reliance are perhaps the perfect agents of a State which would like its population to internalise and individualise their distress, to look to themselves for solutions and to suppose that the reason some people have yachts and others have bailiffs is because some people have more personal skills: far from a balanced perspective.
There is a third set of arguments, and they have recently been brought into a sharp focus. Recovery In The Bin is a Facebook-based survivor group, growing in membership and influence. This month they presented at the Making Sense of Mad Studies conference at Durham University. Members have designed another star, the UnRecovery Star (right). UnRecovery is a term which they define in a number of precise ways. It is a project which continues to evolve. Their attack is a political one: far from opening the frames of reference from narrow medical illness to more holistic personal wellbeing, the Recovery Star continues an onslaught of neoliberalism in mental health, in which people are to be made individually responsible for difficulties which would be better thought of as originating in society. Through this lens, the holism of the Recovery Star becomes a complete colonisation of a person with a set of ideas that appear to be liberating but in fact absolve the powerful from the need to acknowledge and address inequalities of all kinds. For example, widening the conversation to include work and financial skills might seem welcome because loss of role, loss of meaningful activity and financial worries are very significant drivers of distress. However, in so doing, we may be failing to notice with the service-user that they live in an unjust society in which finding one’s way and having access to decent housing, meaningful roles, security, having protected rights and simply being allowed to be different seem to be increasingly the domain of the privileged. Being valued in society may be based on assumptions which many nurses may readily agree are insane. Nurses who unquestionably agree with the Recovery Star that mental health is synonymous with self-reliance are perhaps the perfect agents of a State which would like its population to internalise and individualise their distress, to look to themselves for solutions and to suppose that the reason some people have yachts and others have bailiffs is because some people have more personal skills: far from a balanced perspective.
Part 2: A Lesson
Some final-year mental health nursing students at a large UK university were given the opportunity to compare the two stars as part of their learning about critical mental health. They were asked to consider what a mental health nurse would be doing differently using each star.
Firstly, it was clear that this was new material for them. No one had heard the word ‘iatrogenic’ before, a fact which contains more than a little irony (while acknowledging that it is a rather technical term and that members of the class had considered the possibility that harm may be caused through poor practice). However, it was not just the terminology that was new: it seemed clear that they had been taught and accepted the mainstream messages of distress being mostly biological and occasionally psychological in origin and therefore their focus was a sphere that began and ended with a person’s body/brain and their immediate thoughts, emotions and behaviour. It was difficult for them to formulate ideas for action – a nursing care plan – with the UnRecovery Star. It all looked like problems they could not do anything about.
However, it was more than this. One student made the connection with the idea of internal or external loci of control. This was more familiar territory for the group, and, through that lens, it seemed they were drawn back to prefer the original star. They felt that the external explanations of distress given by the UnRecovery Star would decrease the possibility for recovery because they would discourage the person from taking responsibility for themselves and ‘owning’ their health. There are several things that could be said about this. The first is that it showed that the students understood that responsibility is at the heart of the difference between the Stars. It also showed that they understood that agency is a key part of this debate. After that, it perhaps depends on what view one takes, on one’s politics. Some might say that their instincts perfectly matched their training as normalising agents of neoliberal individualism, being unable to imagine a mental health which was not also making people ultimately responsible for their experiences, and making individuals the only place where change should be brought forth. Under such a view one might notice that as soon as responsibility and change were placed outside of the individual, the student nurses simply had no ideas, no plans, no sense of what could be done about anything and a strong sense that thinking in this way was unhealthy. Accustomed to imagining themselves and their work as apolitical they did not have language to start discussing actions and values such as campaigning and solidarity, empowerment, advocacy, equality and rights. We were not able to move on to any discussion in which we considered what it would be like for a service user to meet either star.
This may all seem rather hard on the student nurses but it seems only right to point out that the exercise revealed that their instinct was to assist people to ‘take responsibility’ for their experiences and they could not easily see how a more social understanding of distress could be turned towards health. Yet the UnRecovery Star was helpful to the students. Through it, they were able to see that the Recovery Star and the individualism it supports is not politically neutral. They might not have had many ideas about how they could work with the UnRecovery Star, but they did view it as missing from standard care and they felt it was an omission that mattered. They agreed with (and were appropriately disturbed by) the thought that a focus on the individual only was in some ways a collusion with direct or systemic abuse and the inequalities of society. They were also able to acknowledge that people in different social situations experienced different kinds and different amounts of choice and that this had a bearing on notions of self-reliance.
As the facilitator, I saw that I share some difficulties with the students. I look into my inner ‘tool box’ and I find that many of the tools are designed to work best in a society which promotes individualism and, yes, recreates health as self-reliance. These tools are not simply wrong but they often further obscure the ways in which I and those around me are formed by society. My experiences of the kinds of possibilities for growth and healing that the solidarity of survivor networks can give, added to the possibilities afforded by the growing number of relationships that I have experienced with people in distress that have placed equality between us as the ‘therapy’, make me feel that it is a difficulty caused by my indoctrination and the stunting of my imagination in a society structured in ways to prevent community and increase alienation. I also feel that I need to constantly remember something I once read in a study relating to the idea of resilience: we are more likely to consider ourselves to be self-reliant when we are surrounded by good social support. This is a conceit I imagine is universal, and one can see how it drives inequality and eases the shift of people towards the right of politics and to prize notions of self-determination as they become more comfortable in life, to discount the significance of the social structures and civil rights that have allowed their individual actions to gain traction.
I think the students shared my feeling that there are no simple answers afforded by keeping both stars in view but that it is essential that we do so and remain feeling uncomfortable. We need to keep thinking about how we may develop skills which would help us use the UnRecovery Star to generate our work.

Interesting article and I am pleased that the work from Recovery in the Bin is coming to critical sites such as this one. I think it important that there is a critique on how Recovery has changed from its initial premises (I believe incorporating aspects of social justice) to how it is currently represented in practice, seemingly focused on promoting self-sufficiency and discharging service users. Like the Facebook site I agree there is a neoliberal influence on care, which could explain the increasing popularity of self-management approaches to promote self-governance in being a ‘worthwhile’ citizen, for example getting a job and not relying on the state. All very well if there is equality in accessing such resources, but as care seemingly confuses autonomy with individualism, there may be times that people need help accessing resources rather than being signposted or having expectation of doing it themselves.
LikeLiked by 1 person
As a retired psychotherapist and former mental health nurse in the NHS, who recently studied Sociology of (mainly mental) health/illness, I would agree with the criticisms of the ‘Recovery Star’. However the UnRecovery star leaves out one important aspect: emotional vulnerability,– frequently arising out of cumulative traumatic experiences in developmental years, perhaps alongside a sensitive nature which was not appreciated or nurtured in the child’s early family/social environment.
This deep vulnerability is carried into adult life with a need to keep this part of self hidden and protected by coping (defence) mechanisms, which impoverish the personality and though felt as necessary for survival, have extremely limiting effects on social interaction. Professionals who work with extremely emotionally vulnerable persons need to recognize this and how our time-poor society in general, being obsessed with celebrity, efficiency, success, has minimal tolerance for such vulnerability, thus reinforcing the need for the sufferer to continue burying that part of themselves which is in such pain.
Such persons can–with the right support–reach some degree of self-reliance, but one that enables them to ASK for emotional support when it is needed; however that can only happen in a social environment which is open to facilitating the expression of such vulnerabilty and also sees the value of .its connection to a wider sensitivity.
It makes me think of a psychological form of the original form of communism: ‘From each according to his ability, to each according to his/her need’. No -one is totally self-reliant.
Ingrid Masterson. RMN; Dip Psychol; former UKCP/ICP Reg Psychotherapist; MSoc Sc.
LikeLiked by 2 people
The terms ‘unrecovery’ and ‘recovery in the bin’ can feel a little pessimistic, as if this movement is saying recovery is not an option. However it only takes a little look into the work coming out of the group, to see that it is not at all pessimistic; it’s a powerful reclamation of the right to work out one’s own route through the challenges that come with mental health difficulties. For too long, professionals have dominated discussions with fairly narrow perspectives on what the future can hold and what options one can take to get there. Life is crappy sometimes and sometimes people don’t recover, certainly not in the terms that proliferate academic literature. This unrecovery star is a great example of how social factors can hugely influence a person’s wellbeing. We need more people standing behind survivor groups, rather than speaking on behalf of service users. I have certainly been guilty of the latter and appreciate reminders such as this to do the former.
LikeLiked by 3 people
I agree with some of the principles on here but it seems to me that the whole idea is full of pessimism. I joined recovery in the bin about a month ago as I was keeping an open mind and trying to see viewpoints from others. However, I found the group to be full of very angry people. The vast majority of the posts in the group were full of hatred towards health professionals, especially nurses.
LikeLike
Being one of the 3rd year students you mention in the article, I’d like to suggest that to have a little more thought provoking conversation regarding the critical approach to mental illness and mental health nursing more time is given. We received only 2 x 2 hour slots that were mainly dominated by you, wanting to cram as much information into them which did not allow much room for discussion. Also, unless you had done your own research into the critical world of psychiatry and mental health nursing, for many students it was a mighty bombshell, it had not been introduced in the circuriculam until the very point they met you. I feel your words for the students were unjust. It is a very emotive subject and more needs to be delivered on this throughout the course not just in 4 hours of a 3 year course!
LikeLiked by 1 person
Hello everyone: Thank you so much for these responses.
Kris: Thanks. The Recovery In the Bin group have been interested in this article and they have been discussing a number of ideas. One of them might be to rename the UnRecovery Star the ‘Social Justice Star’ for the kind of use that we put it to in the class.
Ingrid: I appreciate your comments too. I am not sure if the the RiTB group view their star as a complete view – it is that ‘balanced or balancing’ question. However, I think that they see ‘trauma’ as encompassing what you have said. Couching trauma as ‘vulnerability’ may be helpful for some but for others recast external issues as internal parts or personal pathologies?
Stephen and Catherine: I think it is important to let your comments stand side by side! Both valid experiences I am sure. I would only add that I find that while we may wonder why they seem so angry, they may be often amazed we seem so calm.
Nicola: I totally agree with your statement and feel it should be read by everyone who reads this post. As I said to you all, it felt plain wrong to try to be doing this in 4 hours. As you say, 4 hours on a 3 year course is nothing, especially as we were trying to bring the whole of what we do as mental health nurses into a much broader critical perspective – the UnRecovery Star was just a part of it. Inevitably, I think you and I probably both came out of the experience feeling it was manic and intense. Maybe it is even abusive. Yours is the fifth cohort I have bought this material to, and originally I had just one 3 hour slot! We are at an uncomfortable time in which nurse education simply does not reflect the reality – a rejected DSM, no chemical imbalance, psychology which is being questioned from all sides and much more. I hope that readers of this post will see a group of students who were willing to allow themselves to think hard and be challenged with ideas which ought not to have been new to them but had been hitherto outside of their awareness. In the week before doing the sessions I was encouraged by a respected academic colleague not to go easy on you and not to shy away from showing you the political context of the material. I freely admit it is brutal. Thoughts anyone?
LikeLiked by 1 person
As you can appreciate, we as students have no control over what is deemed needed to qualify in the profession and therefore we can only do what is requested and required. We can, within that time raise issues and concerns regarding the context of the course which many of us do 😊. There are many areas to critique in mental health and how we should best practice to help people who are in distress to help move forward to somewhere close to where they want to be in their own lives. Yes, social factors influence people’s lives both fairly and many unfairly, and can have a huge impact on people’s emotions and I as a soon to be qualified mental health nurse, I want to be able fulfill that role for what I see as its purpose: to provide a valuable presence at the most vulnerable time needed, that will prove to be beneficial. Yes I cannot independently fight the unjust of the world we live in, however, I want to be able to help somebody be in a time of distress and I don’t mean by agreeing to give them medication as let’s face it, I won’t have much choice in that for now but by offering an open mind, to listen, to show empathy and to disagree when I feel that what’s is happening to people in certain element of their care could be given from a different angle and perspective. What my battle is now after your lectures; how is it possible to do this knowing that some elements of mental health nursing could be causing more harm than good? This is what I felt is lacking, how we do this?
LikeLike
Hi Nicola (and Jonathon)
It may be that Jonathon can claim some success by the sheer fact you are having these reflections. It’s my view that the early stages of the ‘battle’ are just embracing these new perspectives; you will be a better, and more critically-minded nurse for it, and it may well influence your thinking and practice in ever-so subtle ways.
I sympathise that there are few obvious ways for a career-minded, newly-qualified nurse to exercise these new understandings, but as a basis for moving upwards through your career into positions of increasing influence, they will be invaluable. Hopefully, along the way, and as you develop in confidence and form your own informed position in the debate, you will encounter a growing range of service-users and colleagues with whom you can test and develop your ideas. I’m fortunate to have developed a local reputation as a polite but vocal thorn-in-the-side of narrow psychiatric framings of our service-users’ complex psychosocial lives. At best, I/we have managed to fully sedgeway our person-centred formulations into multi-disciplinary discussion, and reclaim the ‘clinical’ narrative; at a rare worst, I’ve probably been thought quaint and ‘got to’ by charismatic lefties that we’d all ‘like’ to be right. I/we still lose therapeutic debates along the way – false clinical hope is still invested in wasteful and potentially harmful psychiatric diagnoses and treatments – but there is still plenty to do, further dialogue to be had, and more consciences to raise. Imagine if you or I have never had that Damascus moment, and were still trusting the simplistic truths laid out in the psychiatric textbooks? (I bloody loved those truths; but not nearly as much as the new possibility-space that opened up with jettisoning them – once I got over the initial crisis!)
Good luck with it!
Adam
LikeLiked by 2 people
Thank you for this brilliant article Jonathan.
I first had suspicions about the legitamacy of the recovery star as a recovery tool when I was first introduced to it in 2009. It did not take too much digging to uncover that it is a redesign of St Mungos housing star, which was promoted as an aid to foster collaborative support planning. However, it became clear that the outcomes stars are also being used to audit progress of our service users, and our work. Right before retendering processes, outcomes stars have been scrutinised by funders in order to pick holes in services and justify paying less for them.
The second point I take issue with around these stars, is victim blaming. Lost your house? It is your fault, try harder. You do not trust anyone because you have been abused as a child? Try harder, it is your fault you are not suceeding. I like to think that our service users are not solely to blame for the life situations they find themselves in. Bearing the blame of such serious incidents cannot be good for self esteem, which paradoxically is one of the areas the star is trying to improve.
Finally, my last concern is the concept of this magic 10, that someone is completely independant with an outcome and does not require support from anyone else, ever. Reflecting on my life, I need support from a childcare provider to go to work. I need support from my partner financially to attend university. I need good quality central government legislation to ensure I am in adequte housing. And I need the whole of society to be accepting of my ethnic background, so I do not face discrimiation on the basis of my surname and can form good social networks. I do not feel that we live in a bubble, and work completely dependant of each other. We all need help from someone or something, and we all support others. It is human nature, and I think by the vey nature of making the standard of a perfect 10 so high, we are making it out of reach for all.
Marie, final year student nurse.
LikeLiked by 1 person
I am a service-user/survivor – I like the ‘Un-recovery Star’ debate – Does it go to show that service-user/survivors are not really supposed to recover until we can challenge all the barriers in our own lives and exercise our rights to defend ourselves? In order to do so, and navigate this minefield, does it also show that we have to be able to use our brains and keep our cool and not go crazy whilst we are doing it – cause otherwise we lose our rights and are not ‘recovered’? I assume it takes a lot for a person to do this – the question is ‘how do we make this easier?’ I think there is a valid role for nurses, other professionals, and of course service-user/survivors advocating for themselves and collectively
LikeLike
I enjoyed reading the initial post and subsequent feedback. It’s interesting that not a lot has changed in the nearly 20-years of nursing that I have experienced in regards to the quality of care that some mental health nurses provide. There are always going to be a multitude of excuses why something doesn’t work, but rarely do mental health nurses identify solutions or are innovative in regard to care delivery.
I am going to disagree with all of the posters on here, as I feel that the recovery star does actually have some merit. I understand the star to provide some level of guidance to clinicians when developing care plans with consumers, rather than seeing the star as a consequentialist tool. Developing interpersonal relationships, trust and the like, will enable the clinician to support the consumer to identify deficits in their environment and facilitate change, if that is required. I don’t believe that consumers need to achieve 10’s in all domains to achieve recovery. There is in-built flexibility to review domains as deficits increase, so I believe that it is the clinician who needs to be flexible rather than the consumer and ‘go with the flow’.
It is also interesting to hear from students who need to be supported in their future nursing careers. I think its easy to ‘blame’ student nurses who don’t support others political views. Everyone still maintains the right to have their own point of view heard and considered. However, it is also useful to understand others point of view and integrate it into their practice.
At the end of the day, it is the consumer who is central to their own recovery. It is the consumer that directs their care and is empowered to choose their own path, identify their own mistakes and celebrate their triumphs. It is critical that the consumer movement actively promotes their own agenda that mental health nurses and educators need to be directed by, and not by the medical profession who have promoted iatrogenesis for centuries!
LikeLike
The recovery star is a tool that may be useful for some people (I found it simplistic and patronising), although it has been massively oversold and is being used inappropriately. The unrecovery star manages to be a micky take while making some very serious points.
I don’t feel that student nurses are being blamed for a lack of balance, the experience described is due to a fault in the course design and lack of “consumer” (seriously?) input into the training.
Why aren’t student nurses being exposed to the different viewpoints of people they will be caring for throughout their training?
Especially as MH nursing is so reliant on building relationships. There is no logic to it. There are plenty of service users/experts by experience/people out there who would like to work with universities to help train RMNs.
Please, build it into courses. Use us. We can help you to prevent some of the problems if you have some insight into our views from the start.
LikeLiked by 1 person
Key point:: ‘MH nursing is so reliant on building relationships’ …….and relationships that, rather than bringing a goal-directed agenda aimed at fixing the person, is more a relationship that supports a sufferer in containing, owning and processing their own experience and so finding their own direction.. Therefore the views of sufferers,and of former patients/clients, are paramount.
Our discipline suffers from the widespread pressures of a time-poor, quick fix attitude that permeates society and most health services, totally the opposite to the needed TIME in relationship.
Ingrid Masterson [former RMN/CPN and retired psychotherapist].
LikeLiked by 1 person
I can see that I’m a few years late entering this discussion. All I would like to say is that I made my own poster a couple of years ago in response to both the Recovery Star and the Unrecovery Star – I took on board the ideas presented by the latter, and ignored everything about the original version except for the shape 😊. I even excluded the term ‘recovery.’ If anyone would like a PDF of my poster, it’s free to use. Just let me know.
LikeLike
Hi Jo, I’d like to see your poster.
LikeLike